 For those of you who haven't been reading the comments, we've been having a spirited discussion about the diet and health of hunter-gatherers here. I brought up the Kuna indians in Panama, who are immune to hypertension, live a good long time, do not gain excess weight, and seem to have less cardiovascular disease and cancer than their city-dwelling cousins. I was hungry for more information about the Kuna lifestyle, so over the last few days, I've dug up every paper I could find on them. The first paper describing their lack of hypertension was published in 1944 and I don't have access to the full text. In 1997, a series of studies began, headed by Dr. Norman Hollenberg at Harvard. He confirmed the blood pressure findings, and collected data on their diet, lifestyle and kidney function. Here's a summary:The Kuna are half hunter-gatherers, half agricultural. They cultivate plantains, corn, cocoa, yucca, kidney beans, and several types of fruit. They trade for sugar, salt, some processed cocoa and miscellaneous other foods. They drink 40+ oz of hot cacao/cocoa per day, some locally produced and some imported. A little-known secret: the Kuna eat an average of 3 oz of donut a week. They also fish and hunt regularly. In the first recent study, published in 1997, the Kuna diet is described as 29% lower in fat than the average US diet (56 g/day), 23% lower in protein (12.2 g), 60% higher in cholesterol, and higher in sodium and fiber. The study doesn't specifically mention this, but the reader is left to infer that 65% of their calories come from carbohydrate. This would be from plantains, corn, yucca, sugar and beans. The fat in their diet comes almost exclusively from coconut, cocoa and fish: mostly saturated and omega-3 fats. In the next study, the picture is slightly different. Their staple stew, tule masi, is described as being 38% fat by calories (from coconut and fish), exceeding the American average. In the final study in 2006, Hollenberg's group used a more precise method of accounting for diet composition than was used in previous attempts. The paper doesn't report macronutrients as a percentage of calories however. I was able to find some clues about their diet composition. First of all, they report the meat consumption of the Kuna at approximately 60 oz per week, mostly from fish. That's 8.6 oz per day, identical to the American average. By putting together the pieces from the later studies, a new picture emerges: a diet high in fish and moderate in protein, moderate in unprocessed fat (especially saturated and omega-3), and moderately high in mostly unprocessed carbohydrate. Here's my interpretation. The Kuna are healthier than their city-dwelling cousins for a number of reasons. They have a very favorable omega3:6 ratio due to seafood, wild game and relatively saturated vegetable fats. Their carbohydrate foods are mostly unprocessed and mostly from non-grain sources. They also live an outdoor life full of sunshine (vitamin D) and exercise. The chocolate may also contribute to their health, as it contains high levels of potentially protective polyphenols. They're healthier than industrialized people because they live more naturally. Another lesson to be learned from the Kuna and other exceptionally healthy indigenous peoples is that the human body can tolerate a large amount of carbohydrate under the right conditions.
For those of you who haven't been reading the comments, we've been having a spirited discussion about the diet and health of hunter-gatherers here. I brought up the Kuna indians in Panama, who are immune to hypertension, live a good long time, do not gain excess weight, and seem to have less cardiovascular disease and cancer than their city-dwelling cousins. I was hungry for more information about the Kuna lifestyle, so over the last few days, I've dug up every paper I could find on them. The first paper describing their lack of hypertension was published in 1944 and I don't have access to the full text. In 1997, a series of studies began, headed by Dr. Norman Hollenberg at Harvard. He confirmed the blood pressure findings, and collected data on their diet, lifestyle and kidney function. Here's a summary:The Kuna are half hunter-gatherers, half agricultural. They cultivate plantains, corn, cocoa, yucca, kidney beans, and several types of fruit. They trade for sugar, salt, some processed cocoa and miscellaneous other foods. They drink 40+ oz of hot cacao/cocoa per day, some locally produced and some imported. A little-known secret: the Kuna eat an average of 3 oz of donut a week. They also fish and hunt regularly. In the first recent study, published in 1997, the Kuna diet is described as 29% lower in fat than the average US diet (56 g/day), 23% lower in protein (12.2 g), 60% higher in cholesterol, and higher in sodium and fiber. The study doesn't specifically mention this, but the reader is left to infer that 65% of their calories come from carbohydrate. This would be from plantains, corn, yucca, sugar and beans. The fat in their diet comes almost exclusively from coconut, cocoa and fish: mostly saturated and omega-3 fats. In the next study, the picture is slightly different. Their staple stew, tule masi, is described as being 38% fat by calories (from coconut and fish), exceeding the American average. In the final study in 2006, Hollenberg's group used a more precise method of accounting for diet composition than was used in previous attempts. The paper doesn't report macronutrients as a percentage of calories however. I was able to find some clues about their diet composition. First of all, they report the meat consumption of the Kuna at approximately 60 oz per week, mostly from fish. That's 8.6 oz per day, identical to the American average. By putting together the pieces from the later studies, a new picture emerges: a diet high in fish and moderate in protein, moderate in unprocessed fat (especially saturated and omega-3), and moderately high in mostly unprocessed carbohydrate. Here's my interpretation. The Kuna are healthier than their city-dwelling cousins for a number of reasons. They have a very favorable omega3:6 ratio due to seafood, wild game and relatively saturated vegetable fats. Their carbohydrate foods are mostly unprocessed and mostly from non-grain sources. They also live an outdoor life full of sunshine (vitamin D) and exercise. The chocolate may also contribute to their health, as it contains high levels of potentially protective polyphenols. They're healthier than industrialized people because they live more naturally. Another lesson to be learned from the Kuna and other exceptionally healthy indigenous peoples is that the human body can tolerate a large amount of carbohydrate under the right conditions.
 At 38% and climbing in 2006, the Pima indians (Akimel O'odham) of Arizona have the highest rate of diabetes of any population in the world. They also have staggering rates of obesity (~70%) and hypertension. Things were very different for them before 1539, when the Spanish first made contact. They lived on an agricultural diet of beans, corn and squash, with wild fish, game meat and plants. As with most native people, they were thin and healthy while on their traditional diet. In 1859, the Pima were restricted to a small fraction of their original land along the Gila river, the Pima Reservation. In 1866, settlers began arriving in the region and diverting the Gila river upstream of the reservation for their own agriculture. In 1869, the river went dry for the first time. 1886 was the last year any water flowed to the Pima Reservation in the Gila river. The Pima had no way to obtain water, and no way to grow crops. Their once productive subsistence economy ground to a halt. Famine ensued for 40 desperate years. The Pima cut down their extensive mesquite forests to sell for food and water. Eventually, after public outcry, uncle Sam stepped in.The government provided the Pima with subsidized "food": white flour, sugar, partially hydrogenated lard, and canned goods. They promptly became diabetic and overweight, and have remained that way ever since. The Pima are poster children for mainstream nutrition researchers in the US for several reasons. First of all, their pre-contact diet was probably fairly low in fat, and researchers love to point out that they now eat more fat (comparable to the average American diet). Another reason is that there's another group of Pima in Mexico who still live on a relatively traditional diet and are much healthier. They are genetically very similar, supporting the idea that it's the lifestyle of the American Pima that's causing their problems. The third reason is that the Mexican Pima exercise more than the Arizona Pima and eat a bit less. I of course agree with the conclusion that their lifestyle is behind their problems; that's pretty obvious. I think most Pima know it too. If they got their water back, maybe things would be different for them.
At 38% and climbing in 2006, the Pima indians (Akimel O'odham) of Arizona have the highest rate of diabetes of any population in the world. They also have staggering rates of obesity (~70%) and hypertension. Things were very different for them before 1539, when the Spanish first made contact. They lived on an agricultural diet of beans, corn and squash, with wild fish, game meat and plants. As with most native people, they were thin and healthy while on their traditional diet. In 1859, the Pima were restricted to a small fraction of their original land along the Gila river, the Pima Reservation. In 1866, settlers began arriving in the region and diverting the Gila river upstream of the reservation for their own agriculture. In 1869, the river went dry for the first time. 1886 was the last year any water flowed to the Pima Reservation in the Gila river. The Pima had no way to obtain water, and no way to grow crops. Their once productive subsistence economy ground to a halt. Famine ensued for 40 desperate years. The Pima cut down their extensive mesquite forests to sell for food and water. Eventually, after public outcry, uncle Sam stepped in.The government provided the Pima with subsidized "food": white flour, sugar, partially hydrogenated lard, and canned goods. They promptly became diabetic and overweight, and have remained that way ever since. The Pima are poster children for mainstream nutrition researchers in the US for several reasons. First of all, their pre-contact diet was probably fairly low in fat, and researchers love to point out that they now eat more fat (comparable to the average American diet). Another reason is that there's another group of Pima in Mexico who still live on a relatively traditional diet and are much healthier. They are genetically very similar, supporting the idea that it's the lifestyle of the American Pima that's causing their problems. The third reason is that the Mexican Pima exercise more than the Arizona Pima and eat a bit less. I of course agree with the conclusion that their lifestyle is behind their problems; that's pretty obvious. I think most Pima know it too. If they got their water back, maybe things would be different for them.
However, the focus on macronutrients sometimes obscures the fact that the modern Pima diet is pure crap. It's mostly processed food with a low nutrient density. It also contains the two biggest destroyers of indigenous health: white flour and sugar. There are numerous examples of cultures going from a high-fat diet to a lower-fat "reservation food" diet and suffering the same fate: the Inuit of Alaska, the Maasai and Samburu of Kenya, tribes in the Pacific Northwestern US and Canada, certain Aboriginal groups, and more. What do they all have in common? White flour, sugar and other processed food. The exercise thing is somewhat questionable as well. True, Mexican Pima exercise 2.5 times more than Arizona Pima, but the Arizona Pima still exercise much more than the average American! Women clock in at 3.1 hours a week, while men come in at a whopping 12.1 hours a week! I am a bike commuter and weight lifter, and even I don't exercise that much. So forgive me if I'm a little skeptical of the idea that they aren't exercising enough to keep the weight off. The history of the Pima is a heart-wrenching story that has been repeated hundreds, perhaps thousands of times all over the world. Europeans bring in white flour, sugar and other processed food, it destroys a native populations' health, and then researchers either act like they don't understand why it happened, or give unsatisfying explanations for it. The Pima are canaries in the coal mine, and we can learn a lot from them. Their health problems resemble those of other poor Americans (and wealthier ones also, to a lesser extent). This is because they are both eating similar types of things. The problem is creeping into society at large, however, as we rely more and more on processed wheat, corn, soy and sugar, and less on wholesome food. Obesity in the US has doubled in the past 30 years, and childhood obesity has tripled. Diabetes is following suit. Life expectancy has begun to diminish in some (poor) parts of the country. Meanwhile, our diet is looking increasingly like Pima reservation food. It's time to learn a lesson from their tragedy.
I've been digging deeper into the health of the Masai lately. A commenter on Chris's blog pointed me to a 1972 paper showing that the Masai have atherosclerosis, or hardening of the arteries. This interested me so I got my hands on the full text, along with a few others from the same time period. What I found is nothing short of fascinating. First, some background. Traditional Masai in Kenya and Tanzania are pastoralists, subsisting on fermented cow's milk, meat and blood, as well as traded food in modern times. They rarely eat fresh vegetables. Contrary to popular belief, they are a genetically diverse population, due to the custom of abducting women from neighboring tribes. Many of these tribes are agriculturalists. From Mann et al: "The genetic argument is worthless". This will be important to keep in mind as we interpret the data. At approximately 14 years old, Masai men are inducted into the warrior class, and are called Muran. For the next 15-20 years, tradition dictates that they eat a diet composed exclusively of cow's milk, meat and blood. Milk is the primary food. Masai cows are not like wimpy American cows, however. Their milk contains almost twice the fat of American cows, more protein, more cholesterol and less lactose. Thus, Muran eat an estimated 3,000 calories per day, 2/3 of which comes from fat. Here is the reference for all this. Milk fat is about 50% saturated. That means the Muran gets 33% of his calories from saturated fat. This population eats more saturated fat than any other I'm aware of. How's their cholesterol? Remarkably low. Their total serum cholesterol is about half the average American's. I haven't found any studies that broke it down further than total cholesterol. Their blood pressure is also low, and hypertension is rare. Overweight is practically nonexistent. Their electrocardiogram readings show no signs of heart disease. They have exceptionally good endurance, but their grip strength is significantly weaker than Americans of African descent. Two groups undertook autopsies of male Masai to look for artery disease. The first study, published in 1970, examined 10 males, 7 of which were over 40 years old. They found very little evidence of atherosclerosis, even in individuals over 60. The second study, which is often used as evidence against a high-fat diet, was much more thorough and far more interesting. Mann et al. autopsied 50 Masai men, aged 10 to 65. The single most represented age group was 50-59 years old, at 13 individuals. They found no evidence of myocardial infarction (heart attack) in any of the 50 hearts. What they did find, however, was coronary artery disease. Here's a figure showing the prevalence of "aortic fibrosis", a type of atherosclerotic lesion: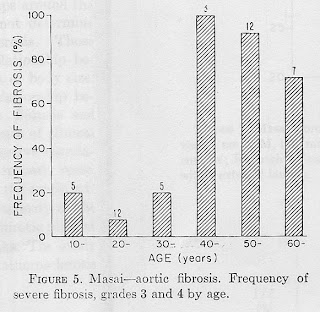 It looks almost binary, doesn't it? What could be causing the dramatic jump in atherosclerosis at age 40? Here's another figure, of total cholesterol (top) and "sudanophilia" (fatty streaks in the arteries, bottom). Note that the Muran period is superimposed (top).
It looks almost binary, doesn't it? What could be causing the dramatic jump in atherosclerosis at age 40? Here's another figure, of total cholesterol (top) and "sudanophilia" (fatty streaks in the arteries, bottom). Note that the Muran period is superimposed (top). 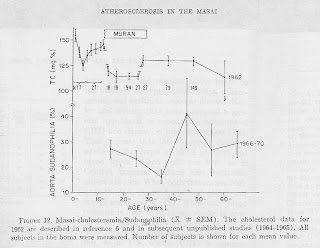 There appears to be a pattern here. Either the Masai men are eating nothing but milk, meat and blood and they're nearly free from atherosclerosis, or they're eating however they please and they have as much atherosclerosis as the average American. There doesn't seem to be much in between. Here's a quote from the paper that I found interesting:
There appears to be a pattern here. Either the Masai men are eating nothing but milk, meat and blood and they're nearly free from atherosclerosis, or they're eating however they please and they have as much atherosclerosis as the average American. There doesn't seem to be much in between. Here's a quote from the paper that I found interesting:
We believe... that the Muran escapes some noxious dietary agent for a time. Obviously, this is neither animal fat nor cholesterol. The old and the young Masai do have access to such processed staples as flour, sugar, confections and shortenings through the Indian dukas scattered about Masailand. These foods could carry the hypothetical agent."
This may suggest that you can eat a wide variety of foods and be healthy, except industrial grain products (particularly white flour), sugar, industrial vegetable oil and other processed food. The Masai are just one more example of a group that's healthy when eating a traditional diet.
I left out one of the juicier tidbits from the last post because it was getting long. Investigators Kang-Jey Ho et al. wanted an explanation for why the Masai didn't have high serum cholesterol despite their high dietary cholesterol intake (up to 2,000 mg per day-- 6.7 times the US FDA recommended daily allowance).
They took 23 male Masai subjects aged 19 to 24 and divided them into two groups. The first group of 11 was the control group, which received a small amount of radioactive cholesterol in addition to a cholesterol-free diet that I will describe below. The second group of 12 was the experimental group, which they fed 2,000 mg cholesterol per day, a small amount of radioactive cholesterol as a tracer, and the exact same cholesterol-free diet as the control group. For the duration of the 24-week trial, the subjects ate the experimental diet exclusively. Here's what it was (in order of calories, descending): - Nondairy coffee creamer (made of corn syrup solids and vegetable oil)
- Beans
- Sugar
- Corn
- Corn oil
- A vitamin pill
Not a healthy diet by most peoples' standards, but those items are nevertheless widely eaten in the US. Over the course of the 24-week study, the investigators found no difference in serum cholesterol between the control and experimental groups. This isn't really surprising. The body has mechanisms for regulating blood cholesterol, and if you aren't eating any it just synthesizes more to stay at its preferred level.
The really interesting thing is that serum cholesterol increased dramatically in both groups. It went from 125 mg/100 mL to over 170 mg/100 mL, despite a large decrease in the saturated fat they were eating. The change took about two weeks to occur, and remained fairly stable for the remainder of the trial.
Both groups also gained weight. In the first week, they gained an average of 3 pounds each. To be fair, the initial gain was probably most water, which is what happens when a person increases their carbohydrate and salt intake. The investigators freaked out and cut their calorie intake by 400 kcal, only allowing them 3,600 kcal per day. Initially, they were voluntarily consuming 4,000 kcal per day. I find that interesting as well. Something tells me they weren't chugging non-dairy creamer because it was so delicious, but because their confused hormones were telling them to EAT.
Even after putting the subjects on calorie restriction (not letting them eat as much as they wanted, by an average of 400 kcal/day), they continued gaining weight. By the end of the study, the 23 subjects had gained an average of 7.8 lbs per person.
To summarize, this is what the investigators saw when they put 23 unfortunate Masai men on a bottom-rung industrially processed diet: elevated cholesterol, hyperphagia (excessive eating), and weight gain. Sounds familiar, doesn't it?
Activator X, the almost-mythical vitamin discovered and characterized by Weston Price, has been identified! For those of you who are familiar with Weston Price's book 'Nutrition and Physical Degeneration', you know what I'm talking about. For the rest of you, allow me to explain. Weston Price was a dentist and scientist in the early part of the 20th century. Practicing dentistry in Cleveland, he was amazed at the poor state of his patients' teeth and the suffering it inflicted. At the time, dental health was even worse than it is today, with some children in their teens already being fitted for dentures. Being a religious man, he could not bring himself to believe that 'physical degeneration' was what God intended for mankind. He traveled throughout the world looking for cultures that did not have crooked teeth or dental decay, and that also exhibited general health and well-being. And he found them. A lot of them. These cultures were all considered 'primitive' at the time, and were not subject to the lifestyles or food choices of the Western world. He documented, numerically and with photographs, the near-absence of dental cavities and crooked teeth in a number of different cultures throughout the world. He showed that like all animals, humans are healthy and robust when occupying the right ecological niche. Price had a deep respect for the nutritional knowledge these cultures curated. He also documented the result when these same cultures were exposed to Western diets of white flour, sugar and other industrially processed foods: they developed rampant cavities, their children grew with crooked teeth due to narrow dental arches, as well as a number of other strikingly familiar health problems. I think it's worth mentioning that Price's findings were universally corroborated by doctors in contact with the same cultures at the time. They are also corroborated by the archaeological record. Many of his findings were published in respected peer-reviewed journals. 'Nutrition and Physical Degeneration' is required reading for anyone interested in the relationship between nutrition and health.Naturally, Price wanted to understand what healthy diets had in common besides the absence of white flour and sugar. Having studied cultures as diverse as the carnivorous Inuit, the dairy-eating Masai and agricultural groups in the Andes, he realized that humans are capable of thriving on very diverse foods. However, he did find one thing in common: they all ate some amount of fat-soluble, animal-derived vitamins. Even the near-vegetarian groups ate insects or small animals that were rich in these vitamins. He looked for, but did not find, a single group that was entirely vegetarian and had the teeth and health of the groups he described in 'Nutrition and Physical Degeneration'. There were three vitamins he found abundantly in the diets of healthy non-industrialized people: A, D, and an unknown substance he called 'activator X'. He considered them all to be synergistic and critical for proper mineral metabolism (tooth and bone formation and maintenance) and general health. He had a chemical test for activator X, but he didn't know its chemical structure and so it remained unidentified. He found activator X most abundantly in grass-fed butter (but not grain fed!), organ meats, shellfish, insects, and fish eggs. Many of these foods were fed preferentially to pregnant or reproductive-age women in the groups he studied. Price used extracts from grass-fed butter (activator X), in combination with high-vitamin cod liver oil (A and D), to prevent and reverse dental cavities in many of his patients. 'Nutrition and Physical Degeneration' contains X-rays of case studies showing re-calcification of severe cavities using this combination. After reading his book, I wasn't sure what to make of activator X. If it's so important, why hasn't it been identified in the 60+ years since he described it? I'm happy to say, it finally has. In the summer of 2007, Chris Masterjohn wrote an article for the Weston Price foundation website, in which he identified Weston Price's mystery vitamin: it's vitamin K2, specifically the MK-4 isoform (menatetrenone).It occurs exactly where Weston Price described it, and research is beginning to find that it's also critical for mineral metabolism, bone and tooth formation and maintenance. Its function is synergistic with vitamins A and D. To illustrate the point, where do A, D and K2 MK-4 all occur together in nature? Eggs and milk, the very foods that are designed to feed a growing animal. This is true from sea urchins to humans, confirming the ubiquitous and critical role of these nutrients. K2 has not yet been recognized as such by the mainstream, but it is every bit as important to health as A and D. The scientific cutting edge is beginning to catch on, however, due to some very tantalizing studies.In the next post, I'll go into more detail about K2, what the science is telling us and where to get it.
Weston Price established the importance of the MK-4 isoform of vitamin K2 (hereafter, K2) with a series of interesting experiments. He showed in chickens that blood levels of calcium and phosphorus depended both on vitamin A and K2, and that the two had synergistic effects on mineral absorption. He also showed that chickens preferred eating butter that was rich in K2 over butter low in K2, even when the investigators couldn't distinguish between them. Young turkeys fed K2-containing butter oil along with cod liver oil (A and D) also grew at a much faster rate than turkeys fed cod liver oil alone. He hypothesized that vitamin A, vitamin D and vitamin K2 were synergistic and essential for proper growth and subsequent health. He particularly felt that the combination was important for proper mineral absorption and metabolism. He used a combination of high-vitamin cod liver oil and high-vitamin butter oil to heal cavities, reduce oral bacteria counts, and cure numerous other afflictions in his patients. He also showed that the healthy non-industrial groups he studied had a much higher intake of these fat-soluble, animal-derived vitamins than more modern cultures. Price found an inverse correlation between the levels of K2 in butter and mortality from cardiovascular disease and pneumonia in a number of different regions. A recent study examined the relationship between K2 (MK-4 through 10) consumption and heart attack risk in 4,600 Dutch men. They found a strong inverse association between K2 consumption and heart attack mortality risk. Men with the highest K2 consumption had a whopping 51% lower risk of heart attack mortality and a 26% lower risk of death from all causes compared to men eating the least K2! Their sources of K2 MK-4 were eggs, meats and dairy. They obtained MK-5 through MK-10 from fermented foods and fish. The investigators found no association with K1, the form found in plants. Perigord, France is the world's capital of foie gras, or fatty goose liver. Good news for the bon vivants: foie gras turns out to be the richest known source of K2. Perigord also has the lowest rate of cardiovascular mortality in France, a country already noted for its low CVD mortality.Rats fed warfarin, a drug that inhibits K2 recycling, develop arterial calcification. Feeding the rats K2 completely inhibits this effect. Mice lacking matrix Gla protein (MGP), a vitamin K-dependent protein that guards against arterial calcification, develop heavily calcified aortas and die prematurely. So the link between K2 and cardiovascular disease is a very strong one. Mammals can synthesize K2 MK-4 from K1 to some degree, so dietary K1 and other forms of vitamin K may contribute to K2 MK-4 status. The synergism Weston Price observed between vitamins A, D and K2 now has a solid mechanism. In a nutshell, vitamins A and D signal the production of some very important proteins, and K2 is required to activate them once they are made. Many of these proteins are involved in mineral metabolism, thus the effects Price saw in his experiments and observations in non-industrialized cultures. For example, osteocalcin is a protein that organizes calcium and phosphorus deposition in the bones and teeth. It's produced by cells in response to vitamins A and D, but requires K2 to perform its function. This suggests that the effects of vitamin D on bone health could be amplified greatly if it were administered along with K2. By itself, K2 is already highly protective against fractures in the elderly. It works out perfectly, since K2 also protects against vitamin D toxicity. I'm not going to go through all the other data on K2 in detail, but suffice it to say it's very very important. I believe that K2 is a 'missing link' that explains many of our modern ills, just as Weston Price wrote. Here are a few more tidbits to whet your appetite: K2 may affect glucose control and insulin release (1, 2). It's concentrated in the brain, serving an as yet unknown function. Hunter-gatherers didn't have multivitamins, they had nutrient-dense food. As long as you eat a natural diet containing some vegetables and some animal products, and lay off the processed grains, sugar and vegetable oil, the micronutrients will take care of themselves.Vitamin K2, MK-4 is only found in animal products. The best sources known are grass-fed butter from cows eating rapidly growing grass, and foie gras. K2 tends to associate with beta-carotene in butter, so the darker the color, the more K2 it contains (also, the better it tastes). Fish eggs, other grass-fed dairy, shellfish, insects and other organ meats are also good sources. Chris Masterjohn compiled a list of food sources in his excellent article on the Weston Price foundation website. I highly recommend reading it if you want more detail. K2 MK-7 is found abundantly in natto, a type of fermented soybean, and it may be partially converted to MK-4.Finally, you can also buy K2 supplements. The best one is butter oil, the very same stuff Price used to treat his patients. I have used this one personally, and I noticed positive effects on my skin overnight. Thorne research makes a synthetic liquid K2 MK-4 supplement that is easy to dose drop-wise to get natural amounts of it. Other K2 MK-4 supplements are much more concentrated than what you could get from food so I recommend avoiding them. I am generally against supplements, but I've ordered the Thorne product for a little self-experimentation. I want to see if it has the same effect on my skin as the butter oil (update- it does).
In Cancer, Disease of Civilization (1960), Wilhjalmur Stefansson mentions a few cultures besides the Inuit in which large-scale searches never turned up cancer. Dr. Albert Schweitzer examined over 10,000 traditionally-living natives in Gabon (West Africa) in 1913 and did not find cancer. Later, it became common in the same population as they began "living more and more after the manner of the whites." In Cancer, its Nature, Cause and Cure (1957), Dr. Alexander Berglas describes the search for cancer among natives in Brazil and Ecuador by Dr. Eugene Payne. He examined approximately 60,000 people over 25 years and found no evidence of cancer. Sir Robert McCarrison conducted a seven year medical survey among the Hunza, in what is now Northern Pakistan. Among 11,000 people, he did not find a single case of cancer. Their diet consisted of soaked and sprouted grains and beans, fruit, vegetables, grass-fed dairy and a small amount of meat (including organs of course).
 The Inuit (also called Eskimo) are a group of hunter-gatherer cultures who inhabit the arctic regions of Alaska, Canada and Greenland. They are a true testament to the toughness, adaptability and ingenuity of the human species. Their unique lifestyle has a lot of information to offer us about the boundaries of the human ecological niche. Weston Price was fascinated by their excellent teeth, good nature and overall robust health. Here's an excerpt from Nutrition and Physical Degeneration:
The Inuit (also called Eskimo) are a group of hunter-gatherer cultures who inhabit the arctic regions of Alaska, Canada and Greenland. They are a true testament to the toughness, adaptability and ingenuity of the human species. Their unique lifestyle has a lot of information to offer us about the boundaries of the human ecological niche. Weston Price was fascinated by their excellent teeth, good nature and overall robust health. Here's an excerpt from Nutrition and Physical Degeneration:"In his primitive state he has provided an example of physical excellence and dental perfection such as has seldom been excelled by any race in the past or present...we are also deeply concerned to know the formula of his nutrition in order that we may learn from it the secrets that will not only aid in the unfortunate modern or so-called civilized races, but will also, if possible, provide means for assisting in their preservation."
The Inuit are cold-hardy hunters whose traditional diet consists of a variety of sea mammals, fish, land mammals and birds. They invented some very sophisticated tools, including the kayak, whose basic design has remained essentially unchanged to this day. Most groups ate virtually no plant food. Their calories came primarily from fat, up to 75%, with almost no calories coming from carbohydrate. Children were breast-fed for about three years, and had solid food in their diet almost from birth. As with most hunter-gatherer groups, they were free from chronic disease while living a traditional lifestyle, even in old age. Here's a quote from Observations on the Western Eskimo and the Country they Inhabit; from Notes taken During two Years [1852-54] at Point Barrow, by Dr. John Simpson:These people [the Inuit] are robust, muscular and active, inclining rather to spareness [leanness] than corpulence [overweight], presenting a markedly healthy appearance. The expression of the countenance is one of habitual good humor. The physical constitution of both sexes is strong. Extreme longevity is probably not unknown among them; but as they take no heed to number the years as they pass they can form no guess of their own ages.
One of the common counterpoints I hear to the idea that high-fat hunter-gatherer diets are healthy, is that exercise protects them from the ravages of fat. The Inuit can help us get to the bottom of this debate. Here's a quote from Cancer, Disease of Civilization (1960, Vilhjalmur Stefansson):"They are large eaters, some of them, especially the women, eating all the time..." ...during the winter the Barrow women stirred around very little, did little heavy work, and yet "inclined more to be sparse than corpulent" [quotes are the anthropologist Dr. John Murdoch, reproduced by Stefansson].
Another argument I sometimes hear is that the Inuit are genetically adapted to their high-fat diet, and the same food would kill a European. This appears not to be the case. The anthropologist and arctic explorer Vilhjalmur Stefansson spent several years living with the Inuit in the early 20th century. He and his fellow Europeans and Americans thrived on the Inuit diet. American doctors were so incredulous that they defied him and a fellow explorer to live on a diet of fatty meat only for one year, under the supervision of the American Medical Association. To the doctors' dismay, they remained healthy, showing no signs of scurvy or any other deficiency (JAMA 1929;93:20–2).Yet another amazing thing about the Inuit was their social structure. Here's Dr. John Murdoch again (quoted from Cancer, Disease of Civilization): The women appear to stand on a footing of perfect equality with the men, both in the family and the community. The wife is the constant and trusted companion of the man in everything except the hunt, and her opinion is sought in every bargain or other important undertaking... The affection of parents for their children is extreme, and the children seem to be thoroughly worthy of it. They show hardly a trace of fretfulness or petulance so common among civilized children, and though indulged to an extreme extent are remarkably obedient. Corporal punishment appears to be absolutely unknown, and children are rarely chided or punished in any way.
Unfortunately, those days are long gone. Since adopting a modern processed-food diet, the health and social structure of the Inuit has deteriorated dramatically. This had already happened to most groups by Weston Price's time, and is virtually complete today. Here's Price:In the various groups in the lower Kuskokwim seventy-two individuals who were living exclusively on native foods had in their 2,138 teeth only two teeth or 0.09 per cent that had ever been attacked by tooth decay. In this district eighty-one individuals were studied who had been living in part or in considerable part on modern foods, and of their 2, 254 teeth 394 or 13 per cent had been attacked by dental caries. This represents an increase in dental caries of 144 fold.... When these adult Eskimos exchange their foods for our modern foods..., they often have very extensive tooth decay and suffer severely.... Their plight often becomes tragic since there are no dentists in these districts.
Modern Inuit also suffer from very high rates of diabetes and overweight. This has been linked to changes in diet, particularly the use of white flour, sugar and processed oils.
Overall, the unique lifestyle and diet of the Inuit have a lot to teach us. First, that some humans are capable of being healthy eating mostly animal foods. Second, that some humans are able to thrive on a high-fat diet. Third, that humans are capable of living well in extremely harsh and diverse environments. Fourth, that the shift from natural foods to processed foods, rather than changes in macronutrient composition, is the true cause of the diseases of civilization.
I bumped into a fascinating paper today by Dr. Loren Cordain titled "Plant-Animal Subsistence Ratios and Macronutrient Estimations in Worldwide Hunter-Gatherer Diets." Published in 2000 in the American Journal of Clinical Nutrition, the paper estimates the food sources and macronutrient intakes of historical hunter-gatherers based on data from 229 different groups. Based on the available data, these groups did not suffer from the diseases of civilization. This is typical of hunter-gatherers.Initial data came from the massive Ethnographic Atlas by Dr. George P. Murdock, and was analyzed further by Cordain and his collaborators. Cordain is a professor at Colorado State University, and a longtime proponent of paleolithic diets for health. He has written extensively about the detrimental effects of grains and other modern foods. Here's his website.The researchers broke food down into three categories: hunted animal foods, fished animal foods and gathered foods. "Gathered foods" are primarily plants, but include some animal foods as well:Although in the present analysis we assumed that gathering would only include plant foods, Murdock indicated that gathering activities could also include the collection of small land fauna (insects, invertebrates, small mammals, amphibians, and reptiles); therefore, the compiled data may overestimate the relative contribution of gathered plant foods in the average hunter-gatherer diet.
There are a number of striking things about the data once you sum them up. First of all, diet composition varied widely. Many groups were almost totally carnivorous, with 46 getting over 85% of their calories from hunted foods. However, not a single group out of 229 was vegetarian or vegan. No group got less than 15% of their calories from hunted foods, and only 2 of 229 groups ate 76-85% of their calories from gathered foods (don't forget, "gathered foods" also includes small animals). On average, the hunter-gatherer groups analyzed got about 70% of their calories from hunted foods. This makes the case that meat-heavy omnivory is our preferred ecological niche. However, it also shows that we can thrive on a plant-rich diet containing modest amounts of quality animal foods.The paper also discusses the nature of the plant foods hunter-gatherers ate. Although they ate a wide variety of plants occasionally, more typically they relied on a small number of staple foods with a high energy density. There's a table in the paper that lists the most commonly eaten plant foods. "Vegetables" are notably underrepresented. The most commonly eaten plant foods are fruit, underground storage organs (tubers, roots, corms, bulbs), nuts and other seeds. Leaves and other low-calorie plant parts were used much less frequently. The paper also gets into the macronutrient composition of hunter-gatherer diets. He writes that ...the most plausible... percentages of total energy from the macronutrients would be 19-35% for protein, 22-40% for carbohydrate, and 28-58% for fat.
He derives these numbers from projections based on the average composition of plant foods, and the whole-body composition of representative animal foods (includes organs, marrow, blood etc., which they typically ate). However, some groups may have eaten more fat than this. Natives on the North American Pacific coast rendered fat from fish, seals, bears and whales, using it liberally in their food. Here's an excerpt from The Northwest Coast by James Swan, who spent three years living among the natives of the Washington coast in the 1850s:About a month after my return from the treaty, a whale was washed ashore on the beach between Toke's Point and Gray's Harbor and all the Indians about the Bay went to get their share... The Indians were camped near by out of the reach of the tide, and were all very busy on my arrival securing the blubber either to carry home to their lodges or boiling it out on the spot, provided they happened to have bladders or barrels to put the oil in. Those who were trying out [rendering] the blubber cut it into strips about two inches wide, one and a half inches thick, and a foot long. These strips were then thrown into a kettle of boiling water, and as the grease tried out it was skimmed off with clam shells and thrown into a tub to cool and settle. It was then carefully skimmed off again and put into the barrels or bladders for use. After the strips of blubber have been boiled, they are hung up in the smoke to dry and are then eaten. I have tried this sort of food but must confess that, like crow meat, "I didn't hanker arter it".
I was very impressed by the paper overall. I think it presents a good, simple model for eating well: eat whole foods that are similar to those that hunter-gatherers would have eaten, including at least 20% of calories from high-quality animal sources. Organs are mandatory, vegetables may not be. Sorry, Grandma.
There are very few cultures left on this planet that have not been affected by modern food habits. There are even fewer that have been studied thoroughly. The island of Kitava in Papua New Guinea is host to one such culture, and its inhabitants have many profound things to teach us about diet and health.
The Kitava study, a series of papers produced primarily by Dr. Staffan Lindeberg and his collaborators, offers a glimpse into the nutrition and health of an ancient society, using modern scientific methods. This study is one of the most complete and useful characterizations of the diet and health of a non-industrial society I have come across. It's also the study that created, and ultimately resolved, my cognitive dissonance over the health effects of carbohydrate.
From the photos I've seen, the Kitavans are beautiful people. They have the broad, attractive faces, smooth skin and excellent teeth typical of healthy non-industrial peoples.
Like the Kuna, Kitavans straddle the line between agricultural and hunter-gatherer lifestyles. They eat a diet primarily composed of tubers (yam, sweet potato, taro and cassava), fruit, vegetables, coconut and fish, in order of calories. This is typical of traditional Pacific island cultures, although the relative amounts differ.
Grains, refined sugar, vegetable oils and other processed foods are virtually nonexistent on Kitava. They get an estimated 69% of their calories from carbohydrate, 21% from fat, 17% from saturated fat and 10% from protein. Most of their fat intake is saturated because it comes from coconuts. They have an omega-6 : omega-3 ratio of approximately 1:2. Average caloric intake is 2,200 calories per day (9,200 kJ). By Western standards, their diet is high in carbohydrate, high in saturated fat, low in total fat, a bit low in protein and high in calories.
Now for a few relevant facts before we really start diving in:
- Kitavans are moderately active. They have an activity level comparable to a moderately active Swede, the population to which Dr. Lindeberg draws frequent comparisons.
- They have abundant food, and shortage is uncommon.
- Their good health is probably not related to genetics, since genetically similar groups in the same region are exquisitely sensitive to the ravages of industrial food. Furthermore, the only Kitavan who moved away from the island to live a modern life is also the only fat Kitavan.
- Their life expectancy at birth is estimated at 45 years (includes infant mortality), and life expectancy at age 50 is an additional 25 years. This is remarkable for a culture with limited access to modern medicine.
- Over 75% of Kitavans smoke cigarettes, although in small amounts. Even the most isolated societies have their modern vices.
The first study in the series is provocatively titled "Apparent absence of stroke and ischaemic heart disease in a traditional Melanesian island: a clinical study in Kitava." In it, Dr. Lindeberg presents data from interviews and electrocardiograms (ECG) suggesting that heart disease and stroke are absent or extremely rare on Kitava. The inhabitants are entirely unfamiliar with the (characteristic) symptoms of heart attack and stroke, despite the sizable elderly population. This is confirmed by the ECG findings, which indicate remarkable cardiovascular health. It also agrees with data from other traditional cultures in Papua New Guinea. Lindeberg states: For the whole of PNG, no case of IHD or atherothrombotic stroke has been reported in clinical investigations and autopsy studies among traditionally living Melanesians for more than seven decades, though an increasing number of myocardial infarctions [heart attacks] and angina pectoris in urbanized populations have been reported since the 1960s.
Dementia was not found except in in two young Kitavans, who were born handicapped. The elderly remained sharp until death, including one man who reached 100 years of age. Kitavans are also unfamiliar with external cancers, with the exception of one possible case of breast cancer in an elderly woman.
Overall, Kitavans possess a resistance to degenerative diseases that is baffling to industrialized societies. Not only is this typical of non-industrial cultures, I believe it represents the natural state of existence for Homo sapiens. Like all other animals, humans are healthy and robust when occupying their preferred ecological niche. Our niche happens to be a particularly broad one, ranging from near-complete carnivory to plant-rich omnivory. But it does not include large amounts of industrial foods.
In the next few posts, I'll discuss more specific data about the health of the Kitavans.
The Kitavans are an isolated population free of cardiovascular disease and stroke, despite the fact that more than three quarters of them smoke cigarettes (although not very frequently). They eat a carbohydrate-heavy, whole-foods diet that is uninfluenced by modern food habits and consists mostly of starchy root crops, fruit, vegetables, coconut and fish. Their intake of grains and processed foods is negligible.Naturally, when Dr. Lindeberg's group discovered that Kitavans don't suffer from heart disease or stroke, they investigated further. In the second paper of the series, they analyzed the Kitavans' "cardiovascular risk factors" that sometimes associate with heart disease in Western populations, such as overweight, hypertension, elevated total cholesterol and other blood lipid markers.Kitavans are lean. Adult male body mass index (BMI) starts out at 22, and diminishes with age. For comparison, Swedes begin at a BMI of 25 and stay that way. Both populations lose muscle mass with age, so Kitavans are staying lean while Swedes are gaining fat. The average American has a BMI of about 28, which is considered overweight and 2 points away from being obese.Kitavans also have a low blood pressure that rises modestly with age. This is actually a bit surprising to me, since other non-industrial groups like the Kuna do not experience a rise in blood pressure with age. Compared with Swedes, Kitavans' blood pressure is considerably lower at all ages.In the next post, I'll discuss the Kitavans' blood lipid numbers ("cholesterol"), which challenge current thinking about heart disease risk factors.
The findings in the previous post are all pretty much expected in a population that doesn't get heart disease. However, things started to get interesting when Lindeberg's group measured the Kitavans' serum lipids ("cholesterol"). Kitavan and Swedish total cholesterol is about the same in young men, around 174 mg/dL (4.5 mmol/L). It rises with age in older Swedish men but not Kitavans. Doctors commonly refer to total cholesterol over 200 mg/dL (5.2 mmol/L) as "high", so Kitavan men are in the clear. On the other hand, Kitavan women should be dying of heart disease left and right with their high middle-age cholesterol of 247 mg/dL (6.4 mmol/L)! That's actually higher than the value for Swedish women of the same age, who are far more prone to heart disease than Kitavans.The fun doesn't stop there. Total cholesterol isn't a good predictor of heart attack risk, but there are better measures. LDL on Kitava is lower in males than in Sweden, but for females it's about the same until old age. HDL is slightly lower than Swedes' at middle and old age, and triglycerides are higher on average. Judging by these numbers, Kitavans should have cardiovascular disease (CVD) comparable to Swedes, who suffer from a high rate of cardiovascular mortality.Kitavan smokers had a lower HDL than nonsmokers, yet still did not develop CVD. Smoking is considered one of the most powerful risk factors for cardiovascular disease in Western populations. I think it's worth noting, however, that Kitavans tend to be light smokers.These data are difficult to reconcile with the hypothesis that certain patterns of blood lipids cause CVD. Kitavans, particularly the women, have a blood lipid profile that should have them clutching their chests, yet they remain healthy. There is a theory of the relationship between blood lipids and CVD that can explain these data. Perhaps blood lipids, rather than causing CVD, simply reflect diet composition and other lifestyle factors. Both on Kitava and in the West, low HDL and elevated triglycerides imply a high carbohydrate intake. Low-carbohydrate diets consistently raise HDL and lower triglycerides. On Kitava, carbohydrate comes mostly from root crops. In the West, it comes mostly from processed grains (typically wheat) and sugar. So the blood lipid pattern that associates best with CVD and the metabolic syndrome in the West is simply a marker of industrial food intake.
The Kitava study continues to get more and more interesting in later publications. Dr. Lindeberg and his colleagues continued exploring disease markers in the Kitavans, perhaps because their blood lipid findings were not consistent with what one would expect to find in a modern Western population with a low prevalence of CVD.In their next study, the researchers examined Kitavans' insulin levels compared to Swedish controls. This paper is short but very sweet. Young Kitavan men and women have a fasting serum insulin level considerably lower than their Swedish counterparts (KM 3.9 IU/mL; SM 5.7; KW 3.5; SW 6.2). Kitavan insulin is relatively stable with age, whereas Swedish insulin increases. In the 60-74 year old group, Kitavans have approximately half the fasting serum insulin of Swedes. One thing to keep in mind is that these are average numbers. There is some overlap between the Kitavan and Swedish numbers, with a few Kitavans above the Swedish mean. In figure 2, they address the possibility that exercise is the reason for Kitavans' low insulin levels. Kitavans have an activity level comparable to a moderately active Swedish person. They divided the Swedes into three categories: low, medium, and high amounts of physical activity at work. The people in the "low" category had the highest insulin, followed by the "high" group and then the "medium" group. The differences were small, however, and Kitavans had far lower serum insulin, on average, than any of the three Swedish groups. These data show that exercise can not explain Kitavans' low insulin levels.The researchers also found that they could accurately predict average Swedish and Kitavan insulin levels using an equation that factored in age, BMI and waist circumference. This shows that there is a strong correlation between body composition and insulin levels, which applies across cultures.Now it's time to take a step back and do some interpreting. First of all, this paper is consistent with the idea (but does not prove) that elevated insulin is a central element of overweight, vascular disease and possibly the other diseases of civilization. While we saw previously that mainstream blood lipid markers do not correlate well with CVD or stroke on Kitava, insulin has withstood the cross-cultural test. In my opinion, the most important finding in this paper is that a high-carbohydrate diet does not necessarily lead to elevated fasting insulin. This is why I think the statement "carbohydrate drives insulin drives fat" is an oversimplification. With a properly-functioning pancreas and insulin-sensitive tissues (which many people in industrial societies do not have), a healthy person can eat a high-carbohydrate meal and keep blood glucose under control. Insulin definitely spikes, but it's temporary. The rest of the day, insulin is at basal levels. The Kitavans show that insulin spikes per se do not cause hyperinsulinemia. So this leads to the Big Question: what causes hyperinsulinemia?? The best I can give you is informed speculation. Who has hyperinsulinemia? Industrial populations, especially the U.S. and native populations that have adopted Western foods. Who doesn't? Non-industrial populations that have not been affected by Western food habits, including the traditional Inuit, the Kuna, the traditional Masai and the Kitavans. We can guess that total fat, saturated fat and carbohydrate do not cause hyperinsulinemia, based on data from the Inuit, the Masai and the Kitavans, respectively. We can also guess that there's not some specific food that protects these populations, since they eat completely different things. Exercise also can not completely account for these findings. What does that leave us with? Western food habits. In my opinion, the trail of metabolic destruction that has followed Westerners throughout the world is probably due in large part to industrial foods, including refined wheat flour, sugar and seed oils.
I'm not the first person to come up with this idea, far from it. The idea that specific types of carbohydrate foods, rather than carbohydrate in general, are responsible for the diseases of civilization, has been around for at least a century. It was an inescapable conclusion in the time of Weston Price, when anthropologists and field physicians could observe the transitions of native people to Western diets all over the world. This information has gradually faded from our collective consciousness as native cultures have become increasingly rare. The Kitava study is a helpful modern-day reminder.
There's a lot to be learned from the Kitava study. Kitavans eat a diet of root vegetables, coconut, fruit, vegetables and fish and have undetectable levels of cardiovascular disease (CVD), stroke and overweight. Despite light smoking. 69% of their calories come from carbohydrate, 21% from fat and 10% from protein. This is essentially a carbohydrate-heavy version of what our paleolithic ancestors ate. They also get lots of sunshine and have a moderately high activity level. The first thing we can say is that a high intake of carbohydrate is not enough, by itself, to cause overweight or the diseases of civilization. It's also not enough to cause insulin resistance. I sent an e-mail to Dr. Lindeberg asking if his group had measured Kitavans' glucose tolerance. He told me they had not. However, I can only guess they had good glucose control since they suffered from none of the complications of unmanaged diabetes. The Kitavan diet is low in fat, and most of the fat they eat is saturated because it comes from coconuts. Compared to Americans and Swedes, they have a high intake of saturated fat. So much for the theory that saturated fat causes CVD... They also have a relatively high intake of fish fat, at 4g per day. This gives them a high ratio of omega-3 to omega-6 fatty acids, with plenty of DHA and EPA. Their blood lipid profile is not what a mainstream cardiologist would expect. In fact, it's "worse" than the Swedish profile in many ways, despite the fact that Swedes are highly prone to CVD. This raises the possibility that blood lipids are not causing CVD, but are simply markers of diet and lifestyle factors. That's very easy for me to swallow because it never made sense to me that our livers would try to kill us by secreting triglycerides and withholding HDL. The blood lipid profile that associates best with CVD and metabolic syndrome in the West (but has no relation to them on Kitava) is one that's consistent with a high carbohydrate intake. Where does carbohydrate come from in the West? White flour and sugar maybe?Kitavans also have very low serum leptin. This may be a keystone to their leanness and health. It suggests that their diet is not interfering with the body's metabolic feedback loops that maintain leanness. The Kitavan diet is one path to vibrant health. Like many other non-industrial groups, Kitavans eat whole, natural foods that are broadly consistent with what our hunter-gatherer ancestors would have eaten. It amazes me that as humans, we can live well on diets that range from near-complete carnivory to plant-rich omnivory. We are possibly the most adaptable species on the planet. The ideal diet for humans includes a lot of possibilities. I believe the focus on macronutrients is misguided. There are examples of cultures that were/are healthy eating high-fat diets, high-carbohydrate diets and everything in between. What they do not eat is processed grains, particularly wheat, refined sugar, industrially processed seed oils and other modern foods. I believe these are unhealthy, and this is visible in the trail of destruction they have left around the globe. Its traces can be found in the Pacific islands, where close genetic relatives of the Kitavans have become morbidly obese and unhealthy on a processed-food diet.
Hunter-gatherers and healthy non-industrial cultures didn't know what omega-6 and omega-3 fats were. They didn't balance nutrients precisely; they stayed healthy by eating foods that they knew were available and nourishing. Therefore, I don't think it's necessary to bean count omega fats, and I don't think there's likely to be a single ideal ratio of n-6 to n-3. However, I do think there's evidence for an optimal range. To find out what it is, let's look at what's been done by healthy cultures in the past:- Hunter-gatherers living mostly on land animals: 2:1 to 4:1
- Pacific islanders getting most of their fat from coconut and fish: 1:2
- Inuit and other Pacific coast Americans: 1:4 or less
- Dairy-based cultures: 1:1 to 2:1
- Cultures eating fish and grains: 1:2 or less
It looks like a healthy ratio is between 4:1 and 1:4 n-6 to n-3. Some of these cultures ate a good amount of n-3 polyunsaturated fat, but none of them ate much n-6 [One rare exception is the !Kung. SJG 2011]. There are three basic patterns that I've seen: 1) low fat with low total n-6 and n-3, and a ratio of less than 2:1; 2) high fat with low total n-6 and n-3 and a ratio of 2:1 or less; 3) high fat with low n-6 and high n-3, and a low carbohydrate intake.I think there's a simple way to interpret all this. Number one, don't eat vegetable oils high in n-6 fats. They are mostly industrial creations that have never supported human health. Number two, find a source of n-3 fats that can approximately balance your n-6 intake. In practical terms, this means minimizing sources of n-6 and eating modest amounts of n-3 to balance it. Some foods are naturally balanced, such as grass-fed dairy and pastured lamb. Others, like coconut oil, have so little n-6 it doesn't take much n-3 to create a proper balance.Animal sources of n-3 are the best because they provide pre-formed long-chain fats like DHA, which some people have difficulty producing themselves. Flax oil may have some benefits as well. Fish oil and cod liver oil can be a convenient source of n-3; take them in doses of one teaspoon or less. As usual, whole foods are probably better than isolated oils. Weston Price noted that cultures throughout the world went to great lengths to obtain fresh and dried marine foods. Choose shellfish and wild fish that are low on the food chain so they aren't excessively polluted.I don't think adding gobs of fish oil on top of the standard American diet to correct a poor n-6:n-3 ratio is optimal. It may be better than no fish oil, but it's probably not the best approach. I just read a study, hot off the presses, that examines this very issue in young pigs. Pigs are similar to humans in many ways, including aspects of their fat metabolism. They were fed three diets: a "deficient" diet containing some n-6 but very little n-3; a "contemporary" diet containing a lot of n-6 and some n-3; an "evolutionary" diet containing a modest, balanced amount of n-6 and n-3; and a "supplemented" diet, which is the contemporary diet plus DHA and arachidonic acid (AA).Using the evolutionary diet as a benchmark, none of the other diets were able to achieve the same fatty acid profile in the young pigs' brains, blood, liver or heart. They also showed that neurons in culture require DHA for proper development, and excess n-6 interferes with the process.With that said, here are a few graphs of the proportion of n-6 in common foods. These numbers all come from nutrition data. They reflect the percentage n-6 out of the total fat content. First, animal fats:.png) Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils:
Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils:.png) These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs:
These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs:.png) n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs. A few of these foods are good sources of n-3. At the top of the list is fish oil, followed by n-3 eggs, grass-fed butter, and the fat of grass-fed ruminants. It is possible to keep a good balance without seafood, it just requires keeping n-6 fats to an absolute minimum. It's also possible to overdo n-3 fats. The traditional Inuit, despite their good overall health, did not clot well. They commonly developed nosebleeds that would last for three days, for example. This is thought to be due to the effect of n-3 on blood clotting. But keep in mind that their n-3 intake was so high it would be difficult to achieve today without drinking wine glasses full of fish oil.
n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs. A few of these foods are good sources of n-3. At the top of the list is fish oil, followed by n-3 eggs, grass-fed butter, and the fat of grass-fed ruminants. It is possible to keep a good balance without seafood, it just requires keeping n-6 fats to an absolute minimum. It's also possible to overdo n-3 fats. The traditional Inuit, despite their good overall health, did not clot well. They commonly developed nosebleeds that would last for three days, for example. This is thought to be due to the effect of n-3 on blood clotting. But keep in mind that their n-3 intake was so high it would be difficult to achieve today without drinking wine glasses full of fish oil.
If Dr. Ancel Keys (of diet-heart hypothesis fame) had been a proponent of "paleolithic nutrition", we would have numerous large intervention trials by now either confirming or denying its ability to prevent health problems. In this alternate reality, public health would probably be a lot better than it is today. Sadly, we have to settle for our current reality where the paleolithic diet has only been evaluated in two small trials, and medical research spends its (our) money repeatedly conducting failed attempts to link saturated fat to every ill you can think of. But let's at least take a look at what we have.Both trials were conducted in Sweden. In the first one, lead by Dr. Per Wändell, 14 healthy participants (5 men, 9 women) completed a 3-week dietary intervention in which they were counseled to eat a "paleolithic diet". Calories were not restricted, only food categories were. Participants were told to eat as much as they wanted of fruit, vegetables, fish, lean meats, nuts, flax and canola oil, coffe and tea (without dairy). They were allowed restricted quantities of dried fruit, potatoes (2 medium/day) salted meat and fish, fat meat and honey. They were told not to eat dairy, grain products, canned food, sugar and salt. After three weeks, the participants had: - Decreased their caloric intake from 2,478 to 1,584 kcal
- Increased their percentage protein and fat, while decreasing carbohydrate
- Decreased saturated fat, increased dietary cholesterol, decreased sodium intake, increased potassium
- Lost 2.3 kg (5 lb)
- Decreased waist circumference, blood pressure and PAI-1
Not bad for a 3-week intervention on healthy subjects. This study suffered from some serious problems, however. #1 is the lack of a control group as a means for comparison. Ouch. #2 is the small study size and resulting lack of statistical power. I consider this one encouraging but by no means conclusive. The second study was conducted by the author of the Kitava study, Dr. Staffan Lindeberg. The study design was very interesting. He randomly assigned 29 men with ischemic heart disease, plus type II diabetes or glucose intolerance, to either a "Mediterranean diet" or a "paleolithic diet". Neither diet was calorie-restricted. Here's the beauty of the study design: the Mediterranean diet was the control for the paleo diet. The reason that's so great is it completely eliminates the placebo effect. Both groups were told they were being assigned to a healthy diet to try to improve their health. Each group was educated on the health benefits of their diet but not the other one. It would have been nice to see a regular non-intervention control group as well, but this design was adequate to see some differences. Participants eating the Mediterranean diet were counseled to focus on whole grains, low-fat dairy, potatoes, legumes, vegetables, fruit, fatty fish and vegetable oils rich in monounsaturated fats and alpha-linolenic acid (omega-3). I'm going to go on a little tangent here. This is truly a bizarre concept of what people eat in the Mediterranean region. It's a fantasy invented in the US to justify the mainstream concept of a healthy diet. My father is French and I spent many summers with my family in southern France. They ate white bread, full-fat dairy at every meal, legumes with fatty pork, sausages and lamb chops. In fact, full-fat dairy wasn't fat enough sometimes. Many of the yogurts and cheeses we ate were made from milk with extra cream added. The paleolithic group was counseled to eat lean meat, fish, fruit, leafy and cruciferous vegetables, root vegetables (including moderate amounts of potatoes), eggs and nuts. They were told to avoid dairy, grain products, processed food, sugar and beer. Both groups were bordering on obese at the beginning of the study. All participants had cardiovascular disease and moderate to severe glucose intolerance (i.e. type II diabetes). After 12 weeks, both groups improved on several parameters. That includes fat mass and waist circumference. But the paleolithic diet trumped the Mediterranean diet in many ways:- Greater fat loss in the the midsection and a trend toward greater weight loss
- Greater voluntary reduction in caloric intake (total intake paleo= 1,344 kcal; Med= 1,795)
- A remarkable improvement in glucose tolerance that did not occur significantly in the Mediterranean group
- A decrease in fasting glucose
- An increase in insulin sensitivity (HOMA-IR)
Overall, the paleolithic diet came out looking very good. But I haven't even gotten to the best part yet. At the beginning of the trial, 12 out of the 14 people in the paleo group had elevated fasting glucose. At the end, every single one had normal fasting glucose. In the Mediterranean group, 13 out of 15 began with elevated glucose and 8 out of 15 ended with it. This clearly shows that a paleolithic diet is an excellent way to restore glucose control to a person who still has beta cells in their pancreas.This post is getting long, so I think I'll save the interpretation for the next post.
In Dr. Lindeberg's paleolithic diet trial, subjects began with ischemic heart disease, and glucose intolerance or type II diabetes. By the end of the 12-week study, on average their glucose control was approaching normal and every subject had normal fasting glucose. Glucose control and fasting glucose in subjects following the "Mediterranean diet" did not change significantly. He didn't report changes in cardiovascular risk factors. Why was the paleolithic diet so effective at restoring glucose control, while the Mediterranean diet was not? I believe the reason is that the Mediterranean diet did not eliminate the foods that were causing the problem to begin with: processed grains, particularly wheat. The paleolithic diet was lower in carbohydrate than the Mediterranean diet (40% vs 52%), although not exceptionally so. The absolute difference was larger since the paleolithic dieters were eating fewer calories overall (134 g vs 231 g). When they analyzed the data, they found that "the effect of the paleolithic diet on glucose tolerance was independent of carbohydrate intake". In other words, paleolithic dieters saw an improvement in glucose tolerance even if they ate as much carbohydrate as the average for the Mediterranean group. This study population is not representative of the general public. These are people who suffered from an extreme version of the "disease of civilization". But they are examples of a process that I believe applies to nearly all of us to some extent. This paper adds to the evidence that the modern diet is behind these diseases. A quick note about grains. Some of you may have noticed a contradiction in how I bash grains and at the same time praise Nutrition and Physical Degeneration. I'm actually not against grains. I think they can be part of a healthy diet, but they have to be prepared correctly and used in moderation. Healthy non-industrial cultures almost invariably soaked, sprouted or sourdough-fermented their grains. These processes make grains much more nutritious and less irritating to the digestive tract, because they allow the seeds to naturally break down their own toxins such as phytic acid, trypsin inhibitors and lectins.Gluten grains are a special case. 12% of the US public is though to be gluten sensitive, as judged by anti-gliadin antibodies in the bloodstream. Nearly a third have anti-gliadin antibodies in their feces [update- these two markers may or may not indicate gluten sensitivity. SJG 2011]. Roughly 1% have outright celiac disease, in which the gut lining degenerates in response to gluten. All forms of gluten sensitivity increase the risk of a staggering array of health problems. There's preliminary evidence that gluten may activate the innate immune system in many people even in the absence of antibodies. From an anthropological perspective, wherever wheat flour goes, so does the disease of civilization. Rice doesn't have the same effect. It's possible that properly prepared wheat, such as sourdough, might not cause the same problems, but I'm not taking my chances. I certainly don't recommend quick-rise bread, and that includes whole wheat. Whole wheat seemed to be enough to preserve glucose intolerance in Lindeberg's study...
I'm always on the lookout for foods rich in vitamin K2 MK-4, because it's so important and so rare in the modern food system. I heard some internet rumors that marrow might be rich in fat-soluble vitamins. Google let me down, so I decided to look through the rat studies on K2 MK-4 in which they looked at its tissue distribution.
I found one that looked at the K2 MK-4 content in different tissues of rats fed vitamin K1. Marrow was rich in K2, along with testes. It contains 10-20 times more MK-4 than liver by weight, and more than any of the other organs they tested (serum, liver, spleen, kidney, heart, testes, marrow, brain) except testes. They didn't include values for salivary gland and pancreas, the two richest sources.
If we assume beef marrow has the same amount of MK-4 as rat marrow per weight (I have no idea if this is really the case, but it's probably in the ballpark), two ounces of beef marrow would contain about 10 micrograms MK-4. Not a huge source, but significant nevertheless.
Bone marrow was a prized food in many hunter-gatherer societies. Let's see what Dr. Weston Price has to say about it (from Nutrition and Physical Degeneration):
For the Indians living inside the Rocky Mountain Range in the far North of Canada, the successful nutrition for nine months of the year was largely limited to wild game, chiefly moose and caribou. During the summer months the Indians were able to use growing plants. During the winter some use was made of bark and buds of trees. I found the Indians putting great emphasis upon the eating of the organs of the animals, including the wall of parts of the digestive tract. Much of the muscle meat of the animals was fed to the dogs. It is important that skeletons are rarely found where large game animals have been slaughtered by the Indians of the North. The skeletal remains are found as piles of finely broken bone chips or splinters that have been cracked up to obtain as much as possible of the marrow and nutritive qualities of the bones. These Indians obtain their fat-soluble vitamins and also most of their minerals from the organs of the animals. An important part of the nutrition of the children consisted in various preparations of bone marrow, both as a substitute for milk and as a special dietary ration.
Here's a bit more about these same groups, also from Nutrition and Physical Degeneration:
The condition of the teeth, and the shape of the dental arches and the facial form, were superb. Indeed, in several groups examined not a single tooth was found that had ever been attacked by tooth decay. In an examination of eighty-seven individuals having 2,464 teeth only four teeth were found that had ever been attacked by dental caries. This is equivalent to 0.16 per cent. As we came back to civilization and studied, successively, different groups with increasing amounts of contact with modern civilization, we found dental caries increased progressively, reaching 25.5 per cent of all of the teeth examined at Telegraph Creek, the point of contact with the white man's foods. As we came down the Stikine River to the Alaskan frontier towns, the dental caries problem increased to 40 per cent of all of the teeth.
Evidently, the traditionally-living groups were doing something right.
Tokelau's troubles began in 1765 with its 'discovery' by British commodore John Byron. Traditionally, residents of the three small coral atolls collectively called Tokelau (Nukunonu, Fakaofo and Atafu) lived an isolated subsistence lifestyle, relying almost exclusively on coconut, seafood, wild fowl and fruit for food. The first reliable account of the Tokelauan population, by an American expedition in 1841, found the people there healthy and happy. Here's an excerpt from Migration and Health in a Small Society: the Case of Tokelau (1992):The expedition considered the people living there to be healthy and handsome... They all appeared to be thriving on their 'meager diet' of fish and coconut, for no evidence of cultivation was seen... People of both sexes were tattooed with geometric designs and figures of turtles and fish. The numerous reports and journals of the Expedition leave the impression of a generally admirable people - amiable (though cautious), peaceful, orderly, and resourceful.
Between 1841 and 1863, the population of Tokelau was reduced to a fraction of its original size by epidemics and kidnapping by slave ships. The old social and religious order was broken, and the inhabitants were converted to Christianity by overzealous and competing Protestant and Catholic missionaries. During this time, Tokelauans also gained new food sources from other Polynesian islands, including breadfruit trees, pulaka (a starchy tuber), pigs and chickens. Breadfruit is a starchy fruit used like plantain.Tokelau became a territory of New Zealand in 1925, and Tokelauans were granted New Zealand citizenship in 1948. In 1963, a government-assisted migration program was established to (voluntarily) bring Tokelauans to the New Zealand mainland, as the population of Tokelau had reached a cozy 1,870 people. When a cyclone devastated coconut and breadfruit crops in 1966, Tokelauans began taking advantage of the assisted migration program in earnest. By 1971, roughly half of Tokelauans lived on the New Zealand mainland.There are two reasons why the Tokelau Island Migrant study is unique. First, it's one of the best-documented transitions from a traditional to a modern lifestyle, studied over decades on Tokelau and in New Zealand. Regular visits by physicians recorded the health of the population as it shifted from a relatively traditional diet to a more Western one. The second thing that makes this population unique is they traditionally have an extraordinarily high saturated fat intake from coconut. They derive between 54 and 62 percent of their calories from coconut, which is 87% saturated. This gives them perhaps the highest documented saturated fat intake in the world. This will be a test of the "diet-heart hypothesis", the idea that dietary fat, cholesterol and especially saturated fat contribute to cardiovascular disease!Through the late 1960s, cargo ships visited Tokelau every three months, making only small contributions to the islanders' diets. In 1968, just two percent of Tokelauans' calories came from sugar. By 1978, the number had risen to 8 percent, and by 1982, 14 percent. The increase came chiefly from refined sugar and sweetened imported foods. In 1961, ships brought 12 lb of flour per person per year to Tokelau, increasing to 60 lb per year by 1980. During this time, importation of low-quality canned meats such as "mutton flaps" and chicken backs, and sweets also increased. Rice imports declined in the 1970s. The diet of migrants to New Zealand rapidly became highly Westernized, containing a higher proportion of refined carbohydrates such as flour and sugar, more red meat and poultry, and less coconut and seafood. Here's a nice quote from Migration and Health in a Small Society: the Case of Tokelau, to set the tone for the rest of the posts in this series:
Here's a nice quote from Migration and Health in a Small Society: the Case of Tokelau, to set the tone for the rest of the posts in this series:
In the mid- and late twentieth century, 'Western diseases'- that is, diseases of affluence (Trowell and Burkitt 1981)- have become the major health risk for Polynesians, because of exposure to cosmopolitan diet patterns and life-style.
The varying cultures and resource bases of islands in the Pacific have influenced the degree to which their populations have been modernized and thus exposed to Western diseases. At one end of the spectrum are relatively traditional subsistence societies such as those on Tokelau and on the low islands- for example Pukapuka, Manihiki, and Rakahanga in the Northern Cook Islands. These atolls are characterized by the almost complete absence of soil, by the inhabitants' dependence on coconut in varied forms, and by a bountiful supply of fish as a major part of the traditional diet. Their populations are notable for their low levels of blood pressure, high rates of infectious disease, and low rates of coronary heart disease, obesity and diabetes. At the other end of the spectrum are those Polynesian societies, such as the Hawaiians and the Maori of New Zealand, who were submerged by 'Western' settlers and the dominating cultures they brought with them. These populations have inevitably acquired the diseases of the 'West', sometimes to an exaggerated degree.
That quote could have been straight out of Nutrition and Physical Degeneration, despite being published 60 years later. Good science is timeless. Join me in future posts as I explore the health of Tokelauan society as it transitions from a traditional diet and lifestyle to a modern one.




.png)
.png)
.png)

{kind=link}